This was a large systematic review that included 69 qualitative studies involving interviews with 1747 patients and clinicians.
Including both patient and clinicians allowed us to compare and contrast views and identify beliefs with confidence.
We used a comprehensive search strategy to identify relevant studies representing the phenomena of interest.
We only included English language studies.
We applied GRADE Confidence in the Evidence from Reviews of Qualitative Research to describe our confidence in the review findings.
Imaging for low back pain is a frequently overused test. In one primary care cohort fewer than 1% of presentations had serious conditions that required immediate imaging.1 Yet physicians refer one in four patients with low back pain presenting to primary care, and one in three patients presenting to emergency care for imaging.2 Imaging is an important diagnostic tool for patients with clinical features of a serious and/or specific condition, such as an infection or spinal cord compromise, and where the results would alter management.3 However, for patients with non-specific low back pain (~95% of presentations in primary care), imaging does not improve outcomes and risks overdiagnosis and overtreatment.4
Overuse of imaging represents a substantial economic burden for low-income, middle-income and high-income countries. In the USA, there were 60 million lumbar radiographs in 2004, around one for every five US citizens5 (out-of-network charges per lumbar radiograph are US$404–US$565).6 In 2016, Australia spent $A243 million7 and Brazil spent US$13 million8 on lumbar radiographs, respectively. In the UK, £77 million was spent on lumbar radiographs in 2000.9 Advanced imaging can be particularly wasteful; a 2016 study of a US Veterans Affairs Healthcare facility estimated US$300 million is wasted on unnecessary lumbar MRIs each year.10
Attempts to reduce overuse of imaging have been largely unsuccessful.11 Although clinicians cite patient pressure and the desire for a definitive diagnosis as a reason for providing guideline-discordant imaging,12 it remains unclear what patients and clinicians believe the role of the imaging test is for people with low back pain. Surveys of patients attending primary care found that nearly 50% believed everyone with low back pain should undergo imaging,13 and 72% rated imaging to be important.14 While such survey studies provide insight into the prevalence of beliefs, they do not explore the underlying reasons for them. Without an in-depth understanding of beliefs about imaging, it will be difficult to design effective strategies to help clinicians manage patient demands and address potential drivers of overuse.
The objective of this review was to synthesise qualitative research that has explored clinician, patient or general public beliefs about diagnostic imaging for low back pain.
We searched MEDLINE, EMBASE, CINAHL, AMED and PsycINFO to locate relevant articles. We did an initial search from inception of each database until 22 September 2017 and updated our search on 17 June 2019. We used a comprehensive sampling strategy.15 To identify additional relevant papers, we conducted a manual search of reference lists of included studies and performed citation tracking of included studies using Web of Science, and contacted experts in the field through authors’ professional networks. Our full search strategy is available in online supplementary appendix 1. We have reported our study according to the Enhancing Transparency in Reporting the synthesis of Qualitative research statement.16 17
Two review authors (ACT and BR) screened titles and abstracts independently and performed a full-text review as necessary. Disagreements were resolved by discussion with a third reviewer (CB).
We included studies if they: used qualitative methods for data collection and analysis; studied clinicians treating low back pain, or patients with any duration of low back pain (who may or may not have received diagnostic imaging), or sampled from the general public and interviewed participants about management of low back pain; explored beliefs about diagnostic imaging for low back pain; were conducted in any healthcare setting in any country; were published in English; and discussed diagnostic imaging of any type (eg, X-ray, CT scan, MRI).
To perform data extraction, three review authors (SS, ACT and CB) independently read a subset of seven included papers that were considered to have rich data on beliefs about imaging. The review authors then developed a preliminary list of themes, using NVivo for theme coding. The review team discussed and revised the preliminary list, and decided on the final list of themes, which then became our coding book. Four authors (ACT, SS, BR and MH) then independently extracted data (such as text extracts and participant quotes) from the included papers and organised these according to the themes and subthemes in the coding book. At least two authors coded each paper. The review team discussed any coding disagreements and agreed on the final organisation of data in the coding book. These steps formed part of the thematic analysis.
We used the Critical Appraisal Skills Programme (CASP) tool to assess the methodological limitations of included studies.18 The CASP tool takes into consideration items such as clarity of the aims, and the appropriateness and rigour of qualitative methods including research design, recruitment strategy, data collection method, consideration of the researcher–participant relationship, ethical issues, data analysis method, clarity of findings, and overall value of the research. Two reviewers (SS and ACT) independently applied the 10-item CASP tool to the included studies.
We summarised the robustness of the review findings following Grading of Recommendations Assessment, Development, and Evaluation (GRADE) Confidence in the Evidence from Reviews of Qualitative Research (CERQual) method.19 To assess confidence in the review findings, two review authors (ACT and SS) independently assessed methodological limitations, relevance, coherence and adequacy of each of the main findings. For a detailed description of this process, please see the online supplement table S1.
We included 69 studies (figure 1), 24 with clinicians (n=630),20–43 32 with patients (n=1072)14 44–74 13 with mixed samples of patients and clinicians (n=45) (table 1).75–87 Detailed characteristics of included studies can be found in online supplementary table S2.
Summary of study characteristics
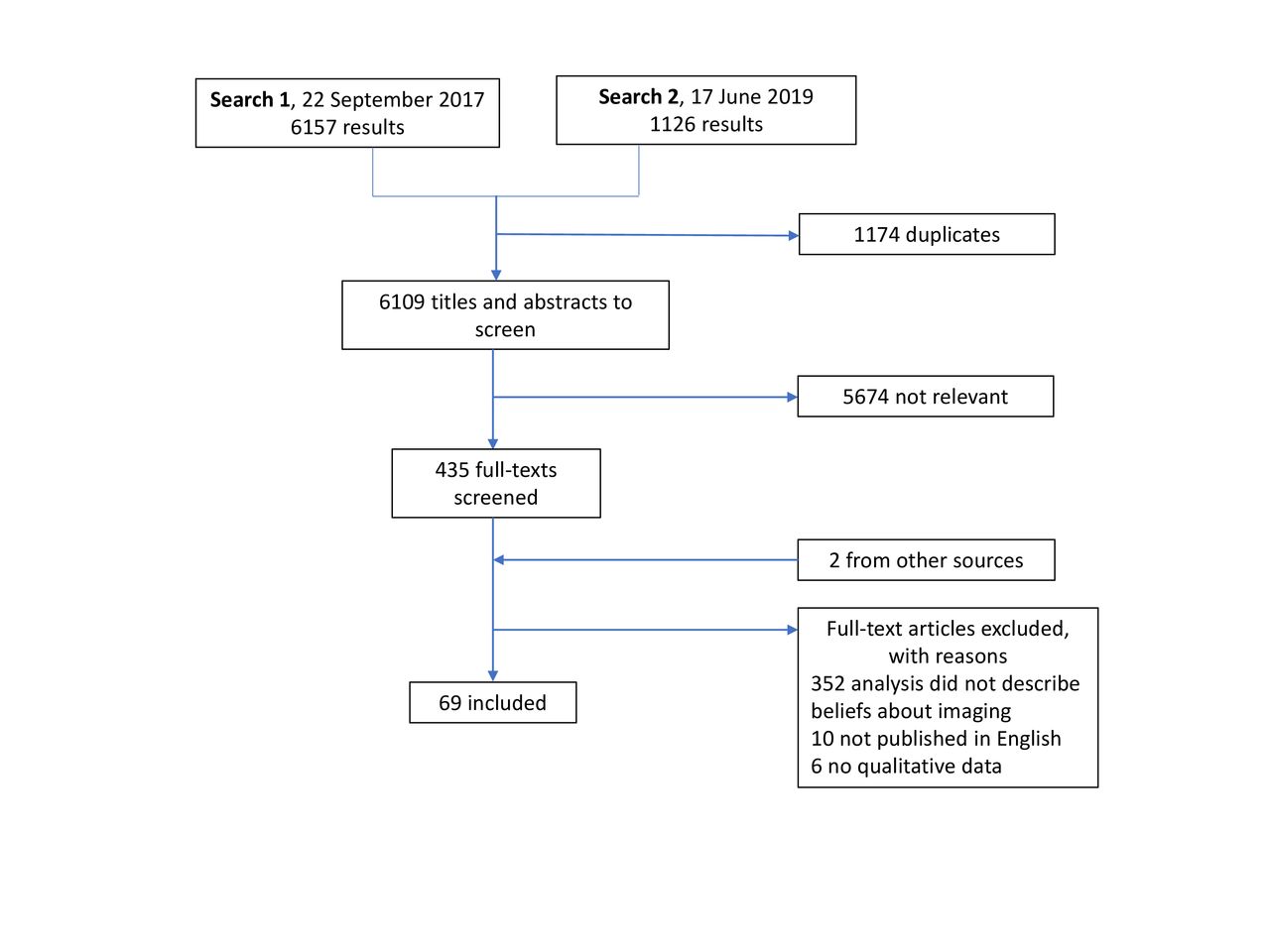
Selection of studies in review of beliefs about diagnostic imaging for low back pain.
Table 2 shows the results of the critical appraisal of included studies. The majority used appropriate qualitative methods (67 of 69, 97%), and research design (66 of 69, 96%). Around half of the studies appropriately reported the researcher–participant relationship (36 of 69, 52%), analysed the data in a rigorous way (32 of 69, 46%) and made a clear statement of their findings (35 of 69, 51%). Less than half of the studies (28 of 69, 41%) had clearly specified their research question and reported collecting data to achieve data saturation (online supplementary table S3).
Critical Appraisal Skill Programme (CASP) assessment of the methodological limitations of included studies
Five major themes emerged from the thematic analysis: (1) Clinical presentation justifies imaging; (2) Perceptions that imaging has benefits to clinicians; (3) Perceptions that imaging has benefits to patients; (4) Imaging has potential harms and (5) Health system drivers. Online supplementary table S4 provides the full list of themes and sub-themes in each study.
Below we describe five main findings based on our thematic analysis and subgroup analyses (figure 2). Based on our CERQual assessment, we found moderate to high confidence in our review findings, with high confidence in two review findings and moderate confidence in three review findings.

Mapping of themes and subthemes to main findings. To summarise our main findings two review authors took the following three steps: (1) review all main analysis and subgroup analyses documents (left side of figure), (2) group findings into key themes and subthemes. (Middle panel) and (3) expand the concise headings of the key theme and sub-theme headings to include a more specific, detailed description of the phenomenon (right side of figure). The summary of findings statements were reviewed and refined by all authors.
This belief arose strongly from the data. Irrespective of the pain duration, patients and clinicians (general practitioners (GPs), chiropractors and physiotherapists) felt it was possible to use diagnostic imaging to locate the source of low back pain. Chiropractors used imaging to assess alignment and guide treatment (eg, identifying which area of the spine to manipulate). Patients and clinicians in all healthcare settings expressed belief that diagnostic imaging is a useful test for non-specific low back pain:
X-rays help me visualize what I am going to do…it is one more piece of information. (Chiropractor)20
They couldn’t quite pick out where it was until the MRIs started and then they found it. (Patient)71
However, some clinicians expressed the contrary belief that imaging is an unreliable tool for locating the source of low back pain:
Well, a lot of them have got a perception [that] X-ray would show things, how they are getting the back problem, and I have to tell them time and time again, the X-ray actually will not show anything really, but this is the perception—it’s generalised. Most of them ask for an X-ray because they think it is a miracle diagnostic tool. It is not. (GP)82
This finding emerged in data from patient participants with chronic low back pain, but not from those with acute low back pain. Patients with chronic low back pain felt the imaging legitimised their pain. They valued the physical evidence of pathology that imaging could provide; results they could use to convince their doctor, family, friends and colleagues that they were in pain. Pathological findings from diagnostic imaging could–paradoxically–bring a sense of relief to patients who felt stigmatised:
I kind of felt relieved. I felt like, well, here’s proof. It’s not just me going crazy or complaining. This is proof. It’s black and white, and anybody can see it. (Patient)63
This theme highlighted the role of diagnosis as a social phenomenon for people with low back pain.
Clinicians in primary care (GPs, chiropractors and physiotherapists) feared missing serious pathology. They mentioned referring patients for imaging even if it was not necessary to reduce the risk of litigation:
I always refer them for x-ray, not because I think there is anything broken, but purely down the line, and the ongoing medico-legal reports, and ‘did you send the patient for x-ray’, and the answer is yes, I have confirmation there is no bony injury. (GP)88
Patients and clinicians believed that negative results provided reassurance to patients:
When patients worry, that is a heavy argument; you need the reassurance (gained from further tests) to go on with the patient. (GP)84
However, negative diagnostic imaging results were not always reassuring; some patient participants expressed frustration if they received results that ‘showed nothing.’ Diagnostic imaging results had the capacity to decrease distress. They could also increase distress if the results were inconclusive or if there were findings perceived to be permanent, degenerative or irreversible. Some clinicians appeared unaware of this negative consequence:
I think if people have a good understanding about where their problem’s coming from in the first place, that for their own piece of mind is a good thing and often they are concerned that what they have is a very serious problem, a life threatening problem and if they’ve got X-rays I explain on their X-rays. (Physio)41
Clinicians focused on potential benefits, such as diagnosing the source of the pain, rather than potential harms such as radiation exposure, increased anxiety and overtreatment. Patients explicitly discussed potential harms in one study and expressed the view that perceived benefits outweighed any harms:
The only downside maybe… was the radiation, but that was the only negative. I think the less radiation you can be exposed to the better, but that having been said, the results justified that risk. I would rely on my doctor’s advice. (Patient)54
Our review suggests that, despite guidelines recommending against the use of diagnostic imaging for non-serious low back pain for over three decades, some clinicians and their patients believe imaging is useful for locating the source of non-specific low back pain. Although clinicians appear to be aware of the downstream consequences of unnecessary imaging, patients rarely considered the potential for harm.
This was a large systematic review that included 69 qualitative studies involving 1747 patients and clinicians. Including both patient and clinicians allowed us to compare and contrast views and identify key beliefs about imaging. We used a comprehensive search strategy to give us the best chance of locating all relevant studies representing the phenomena of interest although a limitation is that we only included English language studies. We adhered to a published protocol, which helps avoid duplication and promote transparency in our work. We applied GRADE CERQual to explain the confidence we had in our review findings.
GRADE CERQual is relatively new and not without limitations. The constructs that inform judgements of confidence in review findings (Methodological Limitations, Relevance, Adequacy, Coherence) can be challenging to measure and open to interpretation. For example, when assessing methodological limitations there is no gold-standard quality assessment tool nor is there specific guidance on including/excluding studies of low quality from reviews. There are also challenges with determining richness and coverage of data to assess Adequacy and Coherence; we acknowledge that a large amount of data does not necessarily guarantee saturation.89
We downgraded confidence in some of our findings for several reasons (online supplementary table S1). In terms of relevance, we included only a few studies primarily aimed to gather beliefs specifically about diagnostic imaging for low back pain. However, in all studies participants freely discussed the management of low back pain, and were given the opportunity to express their beliefs. In terms of adequacy, we located quotes relevant to beliefs that together provided rich data. We included studies with rehabilitation physicians, surgeons and occupational therapists as part of multidisciplinary teams, but were not able to separate quotes from these subgroups in the primary studies. This, we felt, reduced the coherence of some of our findings. However, the themes that emerged from studies of multidisciplinary teams were broadly consistent with the beliefs of the primary care physicians.
We did not find any qualitative studies examining general public beliefs about imaging for low back pain, but they are likely reflected in the beliefs of patients with low back pain who participated in the included studies. We also did not identify qualitative studies that examined beliefs of other specialists that commonly manage people with low back pain depending on setting, such as spine surgeons and other interventionalists. Understanding how closely their beliefs align with primary care clinicians is an important gap in the literature.
Other reviews of qualitative studies that focused on the experience of chronic pain found patients had a strong desire for a medical diagnosis in order to validate their pain.90–94 Toye et al identified a cultural need for a credible explanation of chronic pain, a need that makes it difficult for patients to give up the desire for a ‘diagnostic grail.’90 Our findings suggest that abandoning the desire for a diagnosis will be further complicated if both clinicians and patients believe that imaging can find the cause of the low back pain and legitimise the pain experience. However, we found that not all beliefs were congruent between patients and clinicians. Similar to a review by Hall et al, we found clinicians believed an absence of serious pathology on imaging provides reassurance to some patients.95 We have shown that this was not always true from the patient’s perspective; some patients with chronic low back pain seemed relieved by the presence of pathology on their imaging results—that is, the diagnostic grail. Indeed, a mega-ethnography by Toye et al found that patients with chronic musculoskeletal pain value having visual ‘proof’ in the form of imaging results to legitimise their invisible pain.94
While clinicians in our review mentioned the potential benefit of imaging to legitimise pain, we found the evidence that they were also aware of unintended harms such as the risk of disease labelling, catastrophising, overdiagnosis or overtreatment. Patients, on the other hand, did not appear to be aware of such harms. Previous reviews have suggested a clinician’s decision to ultimately pursue imaging is influenced by several complex factors including a belief that imaging is reassuring,95 misconceptions about clinical guidelines,12 and a desire to satisfy the patient.96 Our review suggests that a mismatch in beliefs and understanding about the harms of imaging could be an important new target for intervention.
A number of studies have evaluated approaches to reduce imaging rates. A Cochrane review97 found that there was little high quality evidence for interventions aimed at clinicians to improve the appropriateness of musculoskeletal imaging. However, there have been limited successes. A trial of providing feedback to GPs on their referral rates reduced imaging rates by 20%.98 Similarly, a 1987 trial found that combined patient education and a delayed referral approach reduced imaging rates by 59%.99 The latter study has never been replicated. Our findings suggest barriers to a delayed referral approach will include (1) a clinician’s belief that imaging is reassuring and (2) a patient’s belief that imaging is routine and can find the source of the pain. These beliefs could be useful targets for future strategies to reduce imaging. In addition, population approaches like mass media campaigns have also been found to shift both societal and clinician beliefs about low back pain towards more evidence-based approaches, although changing behaviours is more challenging.100–102 Population approaches, which have the advantage of simultaneously changing societal beliefs as a whole, remain an underused strategy that could enhance more targeted approaches.
Beliefs about harms of imaging were much less frequently mentioned than beliefs about benefits of imaging. These beliefs are at odds with evidence that diagnostic imaging often adds little value to clinical decision making or patient outcomes. Therefore, these findings suggest a number of valuable areas for future inquiry. Education strategies for all clinicians who manage low back pain (GP, physiotherapists, chiropractors, specialists) are needed to address the widespread belief that imaging can reliably locate the source of low back pain. To address the role of imaging as a social phenomenon for people with low back pain, clinicians require strategies to legitimise a person’s pain experience without the use of diagnostic tests. Interventions to reduce guideline discordant imaging for low back pain should also consider potential social drivers of overuse such as clinician fear of litigation, patient expectations and the need for reassurance (figure 2). Such interventions might include targeted communication materials for the waiting room to address patient expectations and support conversations about the benefits and harms of these tests (box 1).
Did you explain the limited ability of lumbar imaging to locate the source of pain?
Did you discuss potential harms of imaging?
Did you explore misperceptions expressed by your patient?
Did you give your patient enough time to discuss their concerns and did they feel listened to, valued and believed?
Clinicians and patients can believe that diagnostic imaging is an important tool for locating the source of low back pain. Patients may underestimate the harms of unnecessary imaging tests. These beliefs could be important drivers of overuse of imaging and key targets for intervention.
E-mail:
Tel: +44 (0) 141 946 6482
Address: Healthcare Skills Training International Ltd
West of Scotland Science Park
Block 7, Kelvin Campus
Glasgow G20 0SP


