This is the first study to summarise the percentage of physical therapy treatment choices for musculoskeletal conditions that agree with management recommendations in evidence-based guidelines and systematic reviews.
We used a systematic approach to identify studies on physical therapy treatment choices and classified recommendations for physical therapy treatments according to evidence-based guidelines and systematic reviews.
Experts provided feedback to help refine our classification, and a second reviewer double checked all the extracted data to ensure accuracy.
The main limitation is that primary studies only reported treatment choices for individual treatments and not for combinations of treatments.
Recommended treatments such as advice and reassurance might not have been documented in clinical notes or listed in a survey because they may be viewed as a routine part of physical therapy; this could have underestimated the percentage of physical therapists that provided recommended treatments.
Musculoskeletal conditions (such as back and neck pain) have remained the leading cause of disability worldwide over the past two decades and the burden is increasing.1 Concerns about the harms of medicines such as opioids, and new evidence on the lack of effectiveness of common surgical procedures have shifted guideline recommendations for musculoskeletal conditions so there is now more explicit recommendation of non-pharmacological treatments such as those provided by physical therapists. For example, the Center for Disease Control and Prevention recommends exercise therapy instead of opioids in the management of chronic pain.2 Similarly, the 2018 Royal Australian College of General Practitioners guideline for the management of hip and knee osteoarthritis discourages opioids and arthroscopy for knee osteoarthritis and recommends aquatic and land-based exercise.3
Physicians often refer patients with musculoskeletal conditions to physical therapy for non-pharmacological care. In the USA, there are nearly 250 000 physical therapists4 and in Australia there are now more practising physical therapists than general practitioners.5 6 It is important to appreciate however that there are a range of non-pharmacological treatments that physical therapists can provide; some such as exercise are recommended in guidelines for musculoskeletal conditions while others such as electrotherapy are recommended against.7
While there has been considerable attention in medicine on whether physicians are providing recommended care, there has been less attention on whether health services that physicians refer for involve recommended care.8 Determining whether physical therapists are providing treatments recommended in evidence-based guidelines when they manage musculoskeletal conditions is an important step towards ensuring evidence-based care across all healthcare settings.
The aim of this systematic review was to summarise the percentage of physical therapy treatment choices for musculoskeletal conditions that agree with management recommendations in evidence-based guidelines and systematic reviews.
This review was conducted in accordance with the ‘Preferred Reporting Items for Systematic Reviews and Meta-Analyses’ statement.9 Due to the size of the review, other research questions in our registered protocol (including physical therapy treatment choices for cardiorespiratory and neurological conditions) will be addressed in separate manuscripts. Other deviations to our registered protocol include using a modified version of the ‘Downs and Black’ checklist to rate study quality and changing the focus from ‘high-value and low-value care’ to ‘recommended and not-recommended care’.
We conducted a comprehensive keyword search in Medline, Embase, Cumulative Index to Nursing and Allied Health Literature, Cochrane Central Register of Controlled Trials, Allied and Complementary Medicine, Scopus and Web of Science, from the earliest record until April 2018. Our search strategy combined terms relating to ‘practice patterns’ and ‘physical therapy’ (online supplementary table 1) and was designed to capture studies investigating physical therapy treatment choices for any condition (as per our registered protocol). We performed citation tracking and reviewed the reference lists of included studies to identify those missed by our initial database search.
Two independent reviewers (JZ and MO) performed the selection of studies by subsequently screening the title, abstract and full text of studies retrieved through our electronic database search. Any disagreements between the two reviewers were resolved through discussion.
We included any study that reported physical therapy treatment choices for musculoskeletal conditions through surveys of physical therapists (with or without vignettes), audits of clinical notes and other methods (eg, surveys of patients). We only included full-text studies in English. There was no restriction on the musculoskeletal condition treated (eg, neck pain, rehabilitation post knee arthroplasty) or practice setting (eg, private, public), but we excluded studies that reported treatment choices for conditions where there were no known effective or ineffective physical therapist-delivered treatments. We also excluded studies that only quantified physical therapists’ use of assessment procedures, outcome measures, referrals, treatments without specifying a target condition, pharmacological treatments (eg, recommending paracetamol) or treatments outside the usual scope of physical therapy practice (eg, injections); and studies where physical therapy treatment choices were unable to be separated from other healthcare providers.
One reviewer (JZ) independently extracted individual study characteristics (eg, condition, country, participant demographics) and percentages that quantified physical therapy treatment choices (see Data synthesis and Analysis sections). A second reviewer (MO) double checked the extracted data to ensure accuracy. Discrepancies were resolved by discussion between the two reviewers and rechecking data against the original citation. We contacted authors when it appeared that relevant data were not reported.
The methodological quality of included studies was assessed independently by two reviewers (JZ and MO) using a modified version of the Downs and Black checklist. Any disagreements between the two reviewers were resolved through discussion. We modified the original 27-item Downs and Black checklist10 and selected eight items that were relevant to studies on treatment choices (online supplementary table 2). For item eight, we considered the following assessments of treatment choices as ‘accurate’: observation, audits of clinical notes, audits of billing codes, treatment recording forms and validated surveys.
The following definitions were used to classify treatments as recommended, not recommended and no recommendation:
Recommended treatments included physical therapy treatments endorsed in well-recognised evidence-based clinical practice guidelines (eg, guidelines from the National Institute for Health and Care Excellence, NICE) or found to be effective in recent systematic reviews. Treatments recommended in guidelines were further categorised as those that ‘must be provided’ (‘core’ treatments) and those that ‘should be considered’. When guidelines specified core treatments, only these treatments were considered ‘recommended’ in our primary analysis (see Treatment choices that involved treatments that were recommended, not recommended and had no recommendation section). Otherwise, treatments that should be considered were accepted as recommended.
Not-recommended treatments included physical therapy treatments not recommended in guidelines or found to be ineffective in recent systematic reviews.
Treatments with no recommendation included physical therapy treatments where guideline recommendations and evidence from systematic reviews was inconclusive, or where treatments had not been investigated in a systematic review.
We used one clinical practice guideline per condition to classify physical therapy treatments (primary guideline) and contacted leading experts to help us select our primary guideline and refine our classification for a number of conditions (see Acknowledgements). If we found a physical therapy treatment that was not mentioned in the primary guideline, we searched in other evidence-based clinical practice guidelines and systematic reviews to inform our classification (online supplementary table 3). We selected recently published high-quality systematic reviews where possible.
Data on physical therapy treatment choices were divided into two main categories (and analysed separately) due to differences in how each category is interpreted:
Interpretation. Surveys completed by physical therapists’ yielded data on the percentage of physical therapists that provide (survey without vignette) or would provide (survey with vignette) a particular treatment for a condition they frequently treat.
Survey without vignette. Physical therapists outlined the treatments they provide for a condition or rated how often they provide a particular treatment for a condition (eg, ‘frequently’; ‘sometimes’; ‘rarely’; or ‘never’). When studies reported how often treatments were provided, we extracted the percentage of treatments that were provided at least sometimes. We combined data when studies separated survey responses by different samples of physical therapists (usually by country or practice setting). Some surveys were completed by a senior physical therapist on behalf of the physical therapy department within a hospital (eg, management following knee arthroplasty).
Survey with vignette. Physical therapists outlined the treatments they would provide for a particular case (vignette). For studies that included multiple vignettes of the same condition, we took an average of physical therapists’ responses across vignettes of equal sample sizes or used data from the vignette with the highest sample size.
Interpretation. These assessment measures (reported as ‘assessed by clinical notes’ in the results tables) yielded data on the percentage of patients that received a particular physical therapy-delivered treatment in a single treatment session or throughout an episode of care (ie, from initial consultation to discharge).
Audits of clinical notes and billing codes were performed retrospectively in the included studies. Treatment recording forms provided similar information to clinical notes, except they were often implemented as part of a study or registry on treatment practices (prospective). Within a study, we combined data across samples that presented with the same condition (eg, physical therapists from different countries treatment low back pain).
We used counts and ranges to summarise study characteristics for each condition. We used medians and IQRs to summarise the percentage of physical therapy treatment choices that involved treatments that were recommended, not recommended and had no recommendation across studies. We provided an overall result for all studies and then separately for individual musculoskeletal conditions (eg, low back pain). Since physical therapists can provide multiple treatments for the same patient, and treatment choices were summarised across studies, the percentage of treatment choices that involved treatments that were recommended, not recommended and had no recommendation do not sum to 100%. For example, 70% of physiotherapists might provide recommended treatments for low back pain, but the same percentage might also provide some treatments that are not recommended or have no recommendation.
Where possible, recommended treatment was based on treatment choices involving all core treatments recommended in guidelines (ie, physical therapists ‘must’ or ‘should’ provide). For example, the NICE guidelines for low back pain recommend that all patients receive advice and education to support self-management, reassurance and advice to keep active.7 Since studies did not report combinations of treatments, we used the lowest value across all core treatments. For example, if 30% of physical therapists provide reassurance and 50% provide advice to stay active, we used 30% as the percentage of treatment choices that involved recommended treatments. This is because no more than 30% of the sample could have provided both reassurance and advice to stay active (core treatments). If guidelines did not mention core treatments or if there were no guidelines for a condition, we used data from the most frequently provided recommended treatment that should be considered or was found to be effective in a systematic review. We used data from the most frequently provided treatment that was not recommended and had no recommendation to provide an estimate of the percentage of physical therapists’ treatment choices that involve at least one treatment that is not recommended and had no recommendation. For studies that reported treatment choices stratified by the duration of symptoms (acute vs chronic) or different settings (inpatient vs outpatient), we used the highest value of treatments that were recommended, not recommended and had no recommendation across the strata. We summarised the percentage of physical therapy treatment choices that were recommended, not recommended and had no recommendation across all musculoskeletal conditions where guidelines recommended core treatments.
We summarised the percentage of physical therapy treatments provided for various conditions within the categories of recommended, not recommended and no recommendation. Treatments that were procedurally similar and had the same recommendation (ie, recommended, not recommended and no recommendation) were grouped together. For example, according to the NICE low back pain guidelines, mobilisation, manipulation and massage should all be ‘considered’.7 Hence, these were grouped as ‘manual therapy’. Studies rarely reported combinations of physical therapy treatments, so we used data from the most frequently provided treatment where appropriate. For example, if 67% of physical therapists provide massage for acute low back pain and 20% provide mobilisation, we used 67% as the best estimate for the percentage of physical therapists that provide manual therapy.
Patients and members of the public were not involved in the design of this study.
After removing duplicates and screening 8567 titles and abstracts and 254 full-texts reports, 94 studies were included (figure 1). Physical therapy treatment choices were investigated for low back pain (n=48 studies),11–58 knee pain (n=10),32 34 57 59–65 neck pain or whiplash (n=11),15 18 32 34 51 66–71 foot or ankle pain (n=5),72–76 shoulder pain (n=7),15 51 77–81 pre or post knee arthroplasty (n=6)46 82–86 (including one study of hip and knee arthroplasty86) and other musculoskeletal or orthopaedic conditions (where treatment choices were only reported in one study or where one of either recommended or not recommended treatments could not be inferred from guidelines or systematic reviews) (n=18).87–104 We contacted 15 authors for data (regarding 18 studies): 12 responded and 5 were able to provide the data we requested (regarding six studies).15 16 22 64 89 100 A summary of study characteristics across conditions is presented in table 1. Characteristics of included studies are presented in online supplementary table 4.
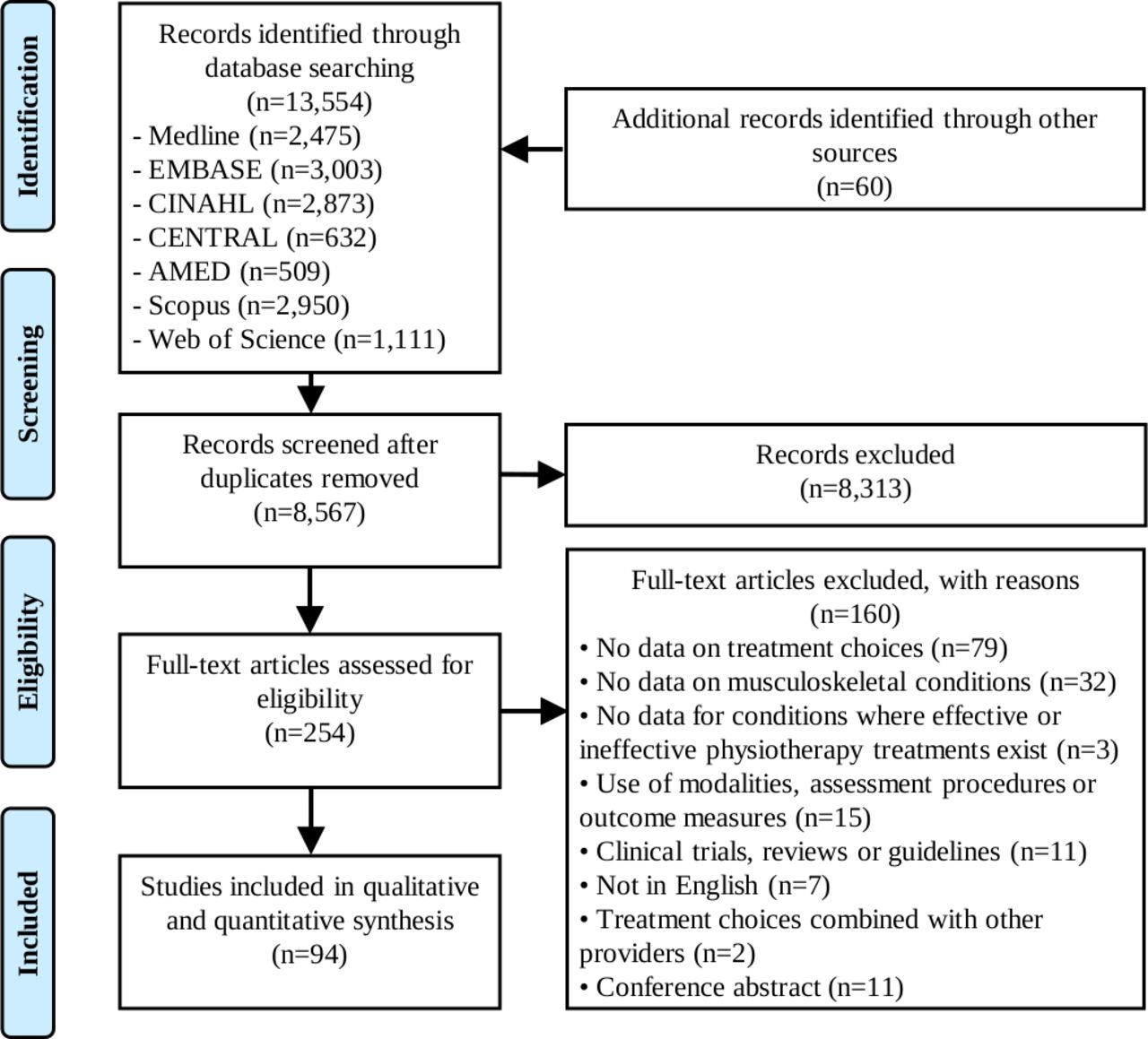
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram. AMED, Allied and Complementary Medicine; CENTRAL, Cochrane Central Register of Controlled Trials; CINAHL, Cumulative Index to Nursing and Allied Health Literature.
Summary of study characteristics by condition
Seven studies investigated treatment choices for shoulder pain: four15 78 80 81 focused on subacromial pain syndrome (the most common form of shoulder pain105), two77 79 included patients with various diagnoses (including subacromial pain syndrome) and one51 did not specify a diagnosis (online supplementary table 4). Evidence on the management of subacromial pain syndrome was used to categorise treatment choices for all studies on shoulder pain. Similarly, evidence on the management of lateral ankle sprains was used to categorise treatment choices for all studies on acute ankle injuries (n=2/3 studies on lateral ankle sprains75 76) and evidence on the management of knee osteoarthritis for all studies on knee pain (excluding one study on acute knee injuries57 and another on a mixed sample of hip and knee osteoarthritis60—see online supplementary table 5).
Individual study scores ranged from 4 to 8 (out of a possible 8) with a mean score of 6.0 (median=6) (online supplementary table 6). The most common methodological limitations included failing to report that physical therapists who were prepared to participate were representative of the population from which they were drawn (n=88/94) and not using an accurate assessment of treatment choices (n=55/94). All studies clearly described their main findings and used appropriate statistical tests, and most scored positive on the remaining checklist items (online supplementary table 6).
The median percentage of physical therapists that provide (or would provide) treatments that were recommended, not recommended and had no recommendation was 54%, 43% and 81% for all musculoskeletal conditions, respectively; 35%, 44% and 72% for low back pain; 85%, 38% and 97% for neck pain and whiplash; 93%, 90% and 79% for shoulder pain; 58%, 45% and 98% for knee pain; 39%, 14% and 7% for lateral ankle sprains; 29%,43% and 98% for plantar fasciitis; and 93%, 52% and 62% following knee or hip arthroplasty (table 2 and figure 2).

Median percentage of physical therapy treatment choices that involved treatments that are recommended, not recommended and had no recommendation. (A) The percentage of physical therapists that report they provide (or would provide) treatments that are recommended, not recommended and had no recommendation for a given condition. (B) The percentage of patients that received treatments that were recommended, not recommended and had no recommendation from a physical therapist for a given condition as determined by audits of clinical notes, audits of billing codes, treatment recording forms, clinical observation or surveys completed by patients. *No treatment choices in this category(s) could be identified. LBP, low back pain; MSK: all musculoskeletal conditions (excluding shoulder pain and knee/hip arthroplasty); OA, osteoarthritis.
Percentage (median and IQR) of physical therapy treatment choices that involved treatments that were recommended, not recommended or had no recommendation
The median percentage of patients that received physical therapy-delivered treatments that were recommended, not recommended and had no recommendation was 63%, 27% and 45% for all musculoskeletal conditions, respectively; 50%, 18% and 43% for low back pain; 79% (not recommended) and 57% (no recommendation) for neck pain and whiplash; 76%, 8% and 62% for shoulder pain; 65%, 21% and 53% for knee pain; 45% (no recommendation) for lateral ankle sprains; 87% (recommended) and 90% (no recommendation) for plantar fasciitis; and 65%, 43% and 2% following knee or hip arthroplasty (table 2 and figure 2).
The results summarising the percentage of physical therapy treatments provided for various musculoskeletal conditions that were recommended, not recommended and had no recommendation can be found in table 3. For example, as assessed by surveys of physical therapists, the most frequently provided recommended treatment for acute low back pain that physical therapists ‘must provide’ was advice to stay active (median=32%, IQR 13%–55%, n=7 studies). The most frequently provided not recommended treatment for acute low back pain was McKenzie therapy (median=36%, IQR 24%–37%, n=6) (table 3). Treatment choices for conditions that were only reported in one study or where one of either recommended or not recommended treatments could not be inferred from guidelines or systematic reviews can be found in online supplementary table 5.
Percentage (median and IQR) of physical therapy treatment choices that involved treatments that were recommended, not recommended or had no recommendation across different conditions
Many physical therapists seem not to follow evidence-based guidelines when managing musculoskeletal conditions. Our review highlights that there is considerable scope to increase the frequency with which physical therapists provide recommended treatments for musculoskeletal conditions and reduce the use of treatments that are not recommended or have no recommendation to guide their use. Across all musculoskeletal conditions, 54% of physical therapists chose recommended treatments, 43% chose treatments that were not recommended and 81% chose treatments that have no recommendation (based on surveys completed by physical therapists). Based on audits of clinical notes, 63% of patients received recommended physical therapy-delivered treatments, 27% received treatments that were not recommended and 45% received treatments that have no recommendation.
The primary strength of this review is that we used a systematic approach to identify studies on physical therapy treatment choices and classified recommendations for physical therapy treatments according to evidence-based guidelines and systematic reviews (online supplementary table 3). Experts provided feedback to help refine our classification, and a second reviewer double checked all the extracted data to ensure accuracy.
The main weakness of this review is that primary studies only reported treatment choices for individual treatments and not combinations of treatments. As a result, we could not determine the percentage of physical therapists that provided only recommended treatments, only not-recommended treatments, only treatments with no recommendation or other combinations of treatments. Second, it is possible that recommended treatments such as advice and reassurance were not documented in clinical notes or listed in a survey because they are viewed as a routine part of physical therapy. For example, only 12 out of the 48 studies on low back pain reported that physical therapists provide advice to stay active, while even less reported reassurance (n=2) or advice and education to support self-management (n=2). This could have underestimated the percentage of recommended treatment choices. Third, physical therapists’ treatment choices may have changed over time so including older studies could limit the relevance of our findings. Nevertheless, we do not believe that this is an important limitation because many guideline recommendations have remained largely consistent overtime. For example, although some studies on treatment choices for low back pain are from 1994, a comparison of low back pain guidelines between 1994 and 2000 found a high degree of consistency of recommendations, such as advice to stay active and avoid bed rest.106 This is consistent with current low back pain guidelines. Finally, most studies did not use an accurate assessment of treatment choices (n=55/94). However, we stratified our analysis by how treatment choices were assessed so the influence of having an accurate method of assessment is clear to readers.
Our finding that approximately half of treatment choices involved recommended treatments is similar to previous studies of healthcare. For example, the CareTrack study in Australia found that 57% of healthcare provided by general practitioners, specialists, physiotherapists, chiropractors, psychologists and counsellors was appropriate,107 while the earlier CareTrack study in the USA found a figure of 55%.108 The percentage of recommended treatment choices for low back pain however was lower in our review (35%–50%) when compared with estimates from the Australian (72%)107 and USA (69%) CareTrack studies.108 A difference to our study is that the CareTrack studies used consensus of experts to judge the value of care, whereas we based this decision on evidence-based practice guidelines and systematic reviews. Another difference is that the CareTrack studies only assessed healthcare decisions through audits of clinical notes; we used audit of clinical notes, surveys, vignettes and clinical observation. Further, the Care Track studies reported primary data collected and were not systematic reviews.
Our results suggest that physical therapy treatment choices for musculoskeletal conditions are often not based on research evidence. There was extensive use of not-recommended treatments and treatments without recommendations; for some conditions, treatments that were not recommended or had no recommendation were more common choices than recommended treatments (figure 2). As there are now over 42 000 clinical practice guidelines, systematic reviews and clinical trials to guide physical therapy practice, the challenge in physical therapy is applying this evidence to practice. Professional associations have a potential role to play in this area. Unfortunately, recent marketing from professional associations, popular social media handles and leading journals have emphasised the importance of early referral to physical therapy109 rather than the nature of physical therapy care provided. The high percentage of non-evidence-based treatment choices in our review suggests that referring patients with musculoskeletal conditions for early physical therapy—without emphasising the importance of the type of non-pharmacological care they receive—may be unwise.
Treatment waste is another important issue highlighted in our review. Even when patients receive recommended treatments, they also usually receive not-recommended treatments and treatments that have no recommendation to guide their use. With nearly US$100 billion spent on physical therapy, optometry, podiatry or chiropractic medicine each year in the USA,110 the waste due to non-evidence-based physical therapy is likely enormous. Further, billing patients for physical therapy treatments that are not evidence based could also be considered unethical; the Vision Statement of the American Physical Therapy Association makes clear that there is an expectation that ‘physical therapists and physical therapist assistants will render evidence-based services’.111
Understanding what drives poor patterns of physical therapy care is important as it will guide the design of strategies to ensure the use of treatments that are not recommended for musculoskeletal conditions does not simply shift from medicine to allied health. One possible explanation is the large variation in physical therapists who receive training in evidence-based practice (21%–82%) and can critically appraise research papers (48%–70%) (systematic review of 12 studies112). Physical therapists with a poor understanding of evidence-based practice might be misled into providing treatments with weak supporting evidence. Another explanation is a lack of awareness of, and agreement with, evidence-based clinical practice guidelines. For example, only 12% of physical therapists are aware of clinical practice guidelines for low back pain (survey of 108 physical therapists)113 and 46% agree that guidelines should inform the management of low back pain (survey of 274 physical therapists).39
A recent initiative that could help physical therapists replace treatments that are not recommended with recommended treatments is Choosing Wisely.114 Over 225 professional societies worldwide endorse Choosing Wisely and have published lists of tests and treatments that clinicians and their patients should question. This includes physical therapy associations in Australia, the USA and Italy. Testing strategies to increase adoption of Choosing Wisely recommendations among physical therapists is important. However, existing Choosing Wisely recommendations are likely not maximising the potential of the campaign to reduce the use of physical therapy treatments that are not recommended in guidelines and systematic reviews. For example, half of the Australian Physiotherapy Association Choosing Wisely recommendations target diagnostic testing that is not recommended, while other recommendations target treatments not part of routine physical therapy care, such as whirlpools for wound management and bed rest following diagnosis of acute deep vein thrombosis (American Physical Therapy Association). Our review highlighted the most frequently provided not-recommended non-pharmacological physical therapy treatments across a range of musculoskeletal conditions (table 3) and could be used to enhance the relevance of future Choosing Wisely recommendations. Further, in countries where physical therapists bill for specific treatments (eg, the USA), another approach could be to restrict funding for anything but recommended physical therapy treatments.
Our results suggest that that there is considerable scope to increase the contribution physical therapists could make to managing musculoskeletal conditions by increasing the frequency with which they provide treatments that are recommended in guidelines and systematic reviews and reduce their use of treatments that are not recommended or have no recommendations to guide their use.
The authors would like to thank Annette Bishop, David Spitaels, Susanne Bernhardsson, David Evans and Melissa Peterson who provided additional data for this study. They would also like to thank Mark Elkins, Rana Hinman, Rachelle Buchbinder, Clair Hiller and Louise Ada for helping them categorise physical therapy treatments as recommended, not recommended and with no recommendation, and Robert Herbert for providing comments on the manuscript.
E-mail:
Tel: +44 (0) 141 946 6482
Address: Healthcare Skills Training International Ltd
West of Scotland Science Park
Block 7, Kelvin Campus
Glasgow G20 0SP


